
Tennis Elbow: What Is and Isn't Helpful for Climbers
Lateral tendon pain (tennis elbow) is considerably more common than medial tendon pain.
It occurs in approximately 10% of the manual labor force, has a high recurrence rate, and does not require treatment to resolve.
Be confident in your natural history
That’s the beauty of natural history! Your body’s amazing at “recovering” on its own. In fact, when researchers compare surgery to physical therapy (all the things) to a wait and see (nothing other than education) intervention, they see similar long-term outcomes!
The strategy really depends on the goals of the individual. If the goals are sports oriented, athletes need higher mechanical loads (heavy and slow) through the process. The ability to tolerate more sport requires greater capacities in the tendons.
What is not helpful for tennis elbow
stretching
deep friction massage
shockwave therapy
low level laser light
electrical stimulation (TENS)
orthosis (bracing)
What might be helpful for tennis elbow
eccentric, concentric, AND isometric loading
nothing (wait and see)
activity modification (regression)
stress reduction / being more social
Mills mobilization (look it up)
cortisone injections ?? (1-2 max)
PRP injections ???? (it’s a coin toss)
The only difference between the rehabilitation (only loading and mills manipulation are supported) and wait and see groups is the speed of symptom resolution, not the long-term health of the tendon. This means that most “therapies” you get are modifying sensitivity, not fixing injuries.
Key takeaways:
If you’re a climber with elbow pain don’t panic. Your pain will go away, whether you like it or not.
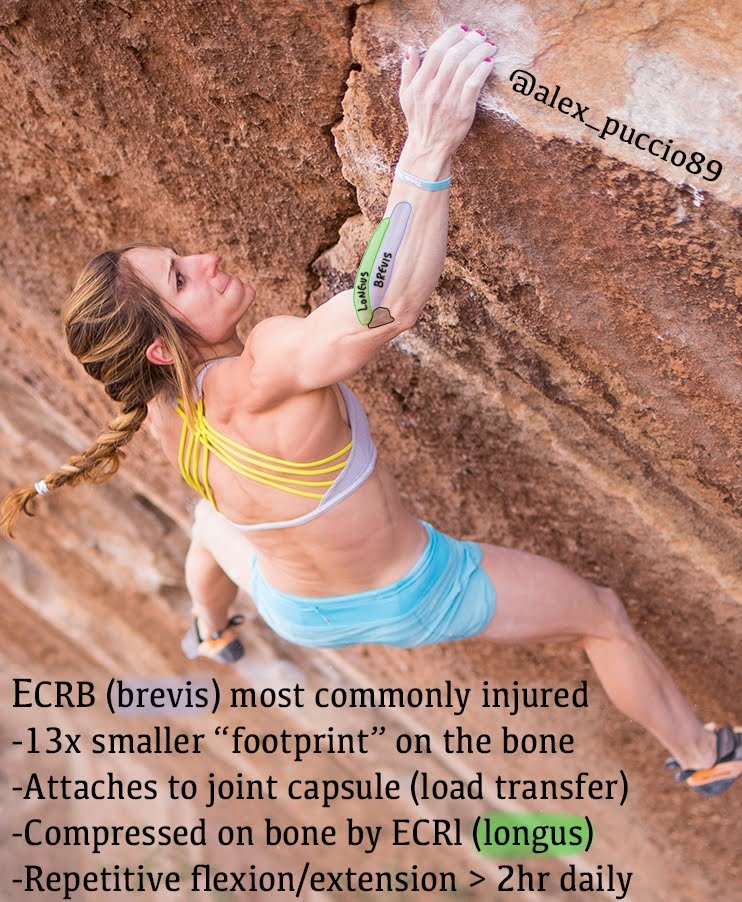
Repetitive flexion at high-velocities and volumes (back hand for tennis players) are likely the primary drivers. If you don’t modify the primary driver of your symptoms you are wasting time and money. Both of which are finite resources.
Be patient, have a training plan, don’t expect a fix (there isn’t one), and be grateful for your bodies ability to adapt.