
Understanding Cubital Tunnel Syndrome in Climbers
Cubital tunnel syndrome is one of the most common compression neuropathies of the upper extremity (literal compression on the nerve).
nothing funny about it.
It is commonly described as pain/tingling/weakness down the inside of the forearm to the pinky and ring fingers.
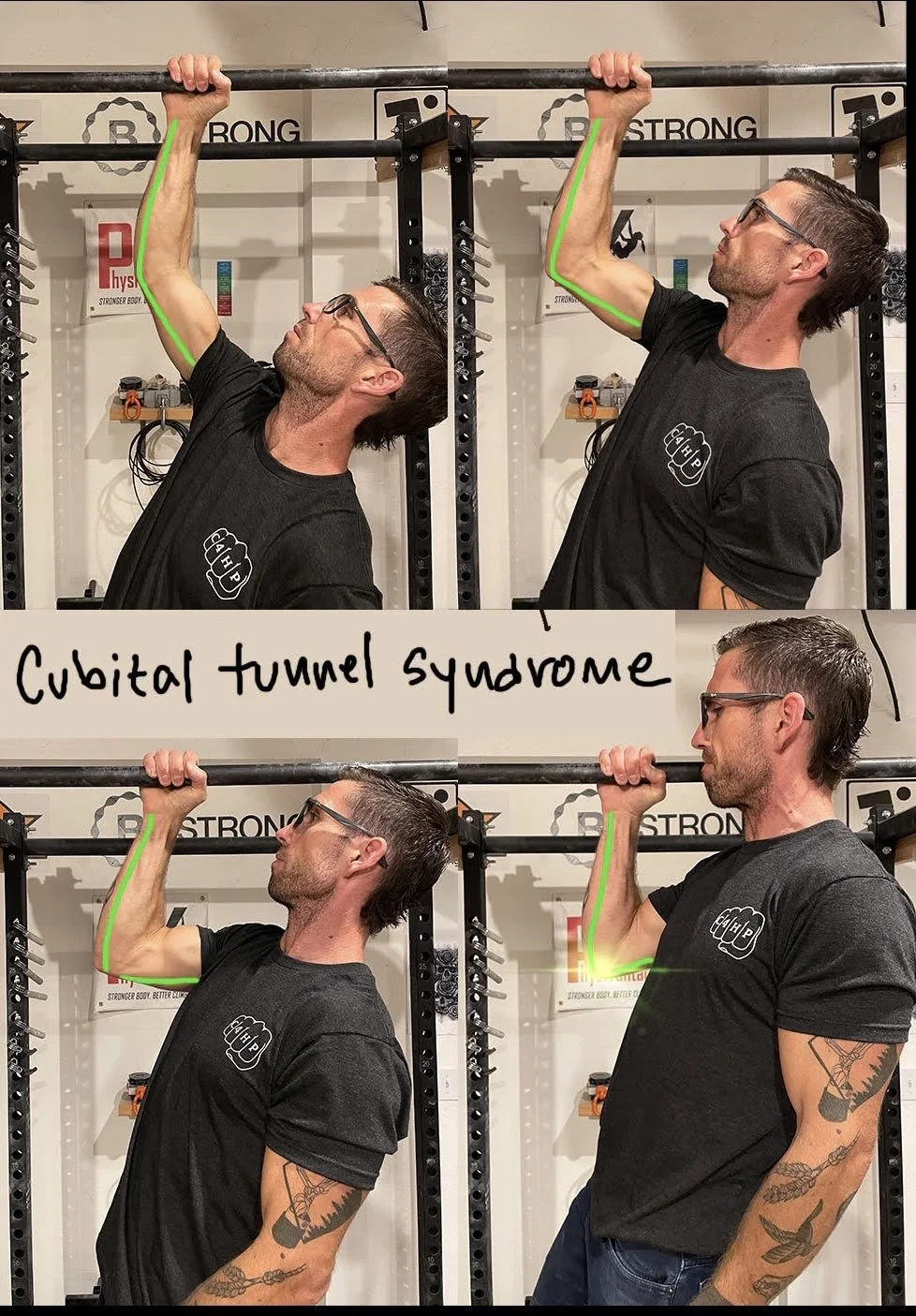
This tunnel is the home of the Ulnar nerve. This nerve passes through the shoulder, down the inside arm, and behind the "funny bone". The real downside for climbers, this nerve is most stressed in fully flexed positions.
treating cubital tunnel syndrome
Even though conservative management is the first line of defense, there isn't good evidence to guide treatment. This is partly due to the suboptimal success rate with surgery. Compared to carpal tunnel (90%), surgical release improves symptoms in 70% of cases.
Because this pathology is irritated with "traction", splints to limit flexion have been the first line of defense for years. The compliance is poor, but that doesn't mean it's not a helpful idea; It's just not practical.
This highlights a significant and obvious intervention, activity modification. Because there are so many "things to do", and "gurus" who do them, the most straightforward interventions get missed.
commonly used non-surgical options include:
Ultrasound-guided steroid injections (helpful mostly)
Nerve glides (useful for sure)
Dry-needling (non-specific, sensory only changes)
Stretching, trigger point therapy (counterproductive)
Laser light therapy (shot in the dark)
Ultrasound (1980's)
what evidence-based healing could look like:
A trial period of 6-12 weeks is a common recommendation.
The most well-supported treatment progression looks something like this. (Note, not all of these are necessary in every case.)
Education/activity modification/regular nerve glides (splinting can also be helpful to reduce traction)
Avoid stretching, compression, tight elbow angles, or exercise which restrict blood flow (BFR).
Ultrasound-guided steroid injections to the cubital tunnel.
Surgical release if conservative management has failed for over 3-6 months.
Key takeaways:
Many treatments aren’t evidence-based.
Activity modification and some non-surgical intervention is often helpful.
“Treatment" doesn't mean routine healthcare visits. Treatment can be education, programming adjustments, and being patient.